Personalising Clinical Documentation at Scale
Improving adoption of ambient AI by designing a self-serve system that let doctors shape their note content from day one.
The editing tax
Suki is an AI-powered healthcare assistant that uses ambient listening to capture clinician–patient conversations and generate clinical documentation automatically. By early 2024, the AI was medically accurate, but physicians are particular about how their notes read and the defaults matched almost nobody.
Physicians were spending 5–10 minutes editing every AI-generated note to match their preferences. In a product whose value is giving doctors time back, that editing overhead was quietly corrosive.
Over 20% of negative feedback the previous quarter cited style mismatch. Formatting complaints dominated: paragraph structure in Assessment and Plan, bullet versus narrative preferences, section-level organisation.
"Sections most often edited: Assessment & Plan: Typically rewritten to match personal style."
"Want Assessment in paragraph form and the problem list should be bulleted."
"The wording of the notes is excessively verbose."
"<Competitor> formats the Assessment and Plan into clean, short paragraphs – much more aligned with my preferred documentation style."
"Notes do not capture encounter reliably, vague"
"Want Assessment in paragraph form and the problem list should be bulleted."
"would be helpful if AI self-learned providers style."
"Sometimes it sounds more like an AP lit class!"
"... want to be in charge of defining which sections they like bulleted and which as a summary (it may vary by patient type and visit type for a single provider)."
"Can I change my templates to make the “diet history” and “exercise” sections appear in bulleted format?"
Our goal was to identify the primary drivers of editing effort and deliver immediate and long-term personalisation strategies that could meaningfully improve note quality, adoption, and trust.
How might we help physicians generate notes that already sound like they wrote them – reducing editing effort while maintaining clinical accuracy and consistency?
30+ interviews with clinicians revealed how time pressure and scepticism toward AI shaped documentation behaviours. These insights would directly inform how we designed our solution for trust, speed, and minimal disruption.

Dr. Reed
Experienced Primary Care Physician evaluating a new documentation tool under time pressure. Highly opinionated about how clinical notes should read and fit into her EHR. Little tolerance for tools that disrupt established workflows.
"As a busy clinician, I want Suki to automatically adapt its output to my unique preferences, so that I can eliminate repetitive, time-consuming manual edits."
Wants to
Motivations
Hates that
Behaviours & mindset
Personalisation is three different things
From the feedback and interviews, we identified three main buckets.
Design-PM-ML brainstorms
Design-PM-ML brainstorms produced 4 core approaches which we discussed with clinicians.
- Low cognitive load – familiar mental model
- Gold standard notes were too hard to source. Most physicians couldn't name one
- Style varies section by section within the same clinician – a single note overfits
- No upfront setup, preserves existing workflow
- Barely a step up from the current editing paradigm. Clinicians still felt like they were fixing
- Shifted the burden without removing it – four interactions per note added up
- Most appealing on paper – zero onboarding effort, improves with use
- Ideal but would take a while to build. ML team was already stretched, two quarters out
- Cold-start remained entirely unsolved. Early mistakes damage trust before learning kicks in
- Highest adoption signal across all twelve clinicians. Clinicians in early onboarding are less busy and more open to configuration – the window exists, and we could use it
- No ML dependency – designable and shippable within the quarter
- Solved cold-start without waiting for behavioural data
- Options need careful curation – too many choices increased time in selection
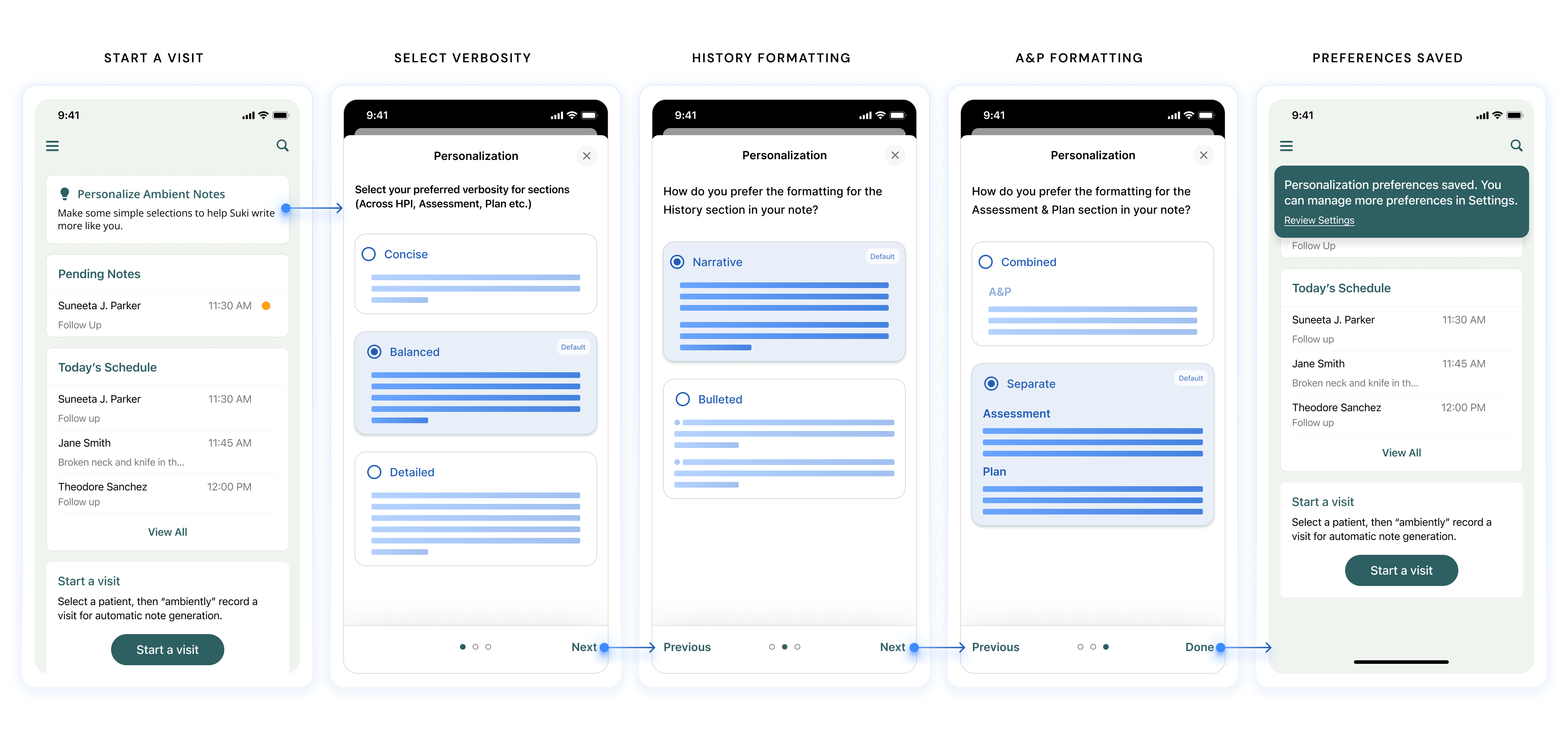
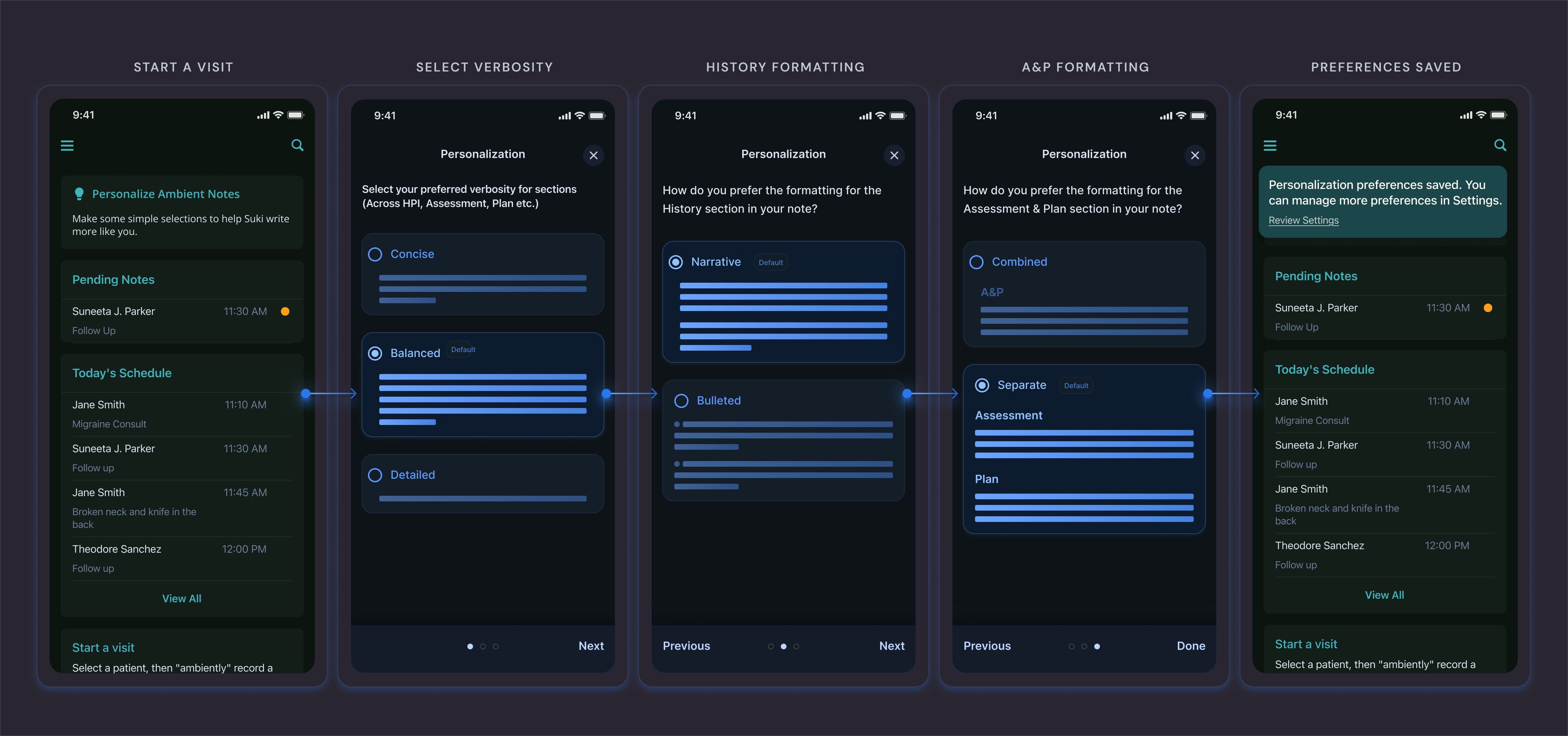
Move personalisation to the front of the experience.
ML could optimise the experience eventually. But solving the cold-start problem required an immediate, non-ML solution.
A one-week pilot with 30 clinicians
We built a linear onboarding flow letting physicians set preferences across a limited set of note sections. Intentionally low-click and setup in two minutes or less. We ran a pilot across 30 net-new clinicians at a single clinical centre over the first week of live use, behind a pilot-only feature flag.
The settings model needed more depth.
Multiple settings define a single note section – format, organisation, and verbosity combine to produce what a physician experiences as 'how my HPI reads.'
Reduce reading time. Show, don't tell for the formatting options.
The task was to expand customisation across the note sections that matter most to clinicians. Because multiple settings shape a single section, preferences needed to group logically to enable targeted changes with minimal effort while helping users understand the overall impact of their choices.
Instances of complex, inter-linked settings being applied across other apps.
Build for scale
- 55-year-old male with hypertension and chronic angina.
- Presents for follow-up.
- Reports new-onset chest pain began 2 weeks ago.
- Described as squeezing pressure, radiating to left jaw.
- Occurs at rest, lasts up to 10 minutes.
- Partially relieved by nitroglycerin.
- Denies shortness of breath or palpitations.
We explored multiple UI options, from dense text to minimal structures, landing on
The minimal horizontal-line representation that kept the design lightweight and easy to scan.
- We built a small set of flexible components that could recombine to support new note sections and specialties without new design work each time.
- Long term, the feature team could add configurations without increasing design or engineering complexity. The same UI held across all specialties.
Section-grouped settings with a live preview
A central settings space where physicians configure note preferences by section, with a live preview that updates as they select.

The settings page is constantly in motion. Sections unfold, previews respond in real time, and selections provide subtle feedback. It was an opportunity to introduce moments of delight and craftsmanship into an otherwise serious, text-heavy product.
To keep the experience cohesive, I documented a set of motion guidelines that defined timing, easing, and the intent behind each interaction.
Solve the cold start
Users received a condensed version of these questions during onboarding. It softened the cold start: a clinician's first note already reflected some of their preferences, instead of arriving with Suki's defaults. The same flow pointed clinicians toward the settings page for anything more specific.